
Anemia Management
Anemia is common in end stage kidney disease and is associated with increased morbidity and mortality related to cardiovascular disease (hypertrophy, heart failure), an increased risk of hospitalization, and symptoms including fatigue and depression. The introduction of erythropoietin (EPO) and erythropoiesis-stimulating agents (ESAs) revolutionized the treatment of anemia in CKD patients by improving anemic symptoms, but there is notable variation in patient EPO responsiveness with a subset of patients exhibiting a poor response1 as well as studies revealing potential risks associated with use of high dose ESA. Alternatively, more frequent HD has also been shown to help with anemia management in ESKD patients by improving hemoglobin and hematocrit levels and reducing the need for EPO1–4.
Daily HD (3-4 hours, 5 times/week) was shown to improve anemia as early as 1972, in the pre-erythropoietin era, with an increase in hematocrit (Hct) from 16 to 24%, and a reduction in blood transfusions from 1.33 to 0.16 units per month (Figure 1)5, despite a shortening of total hours of dialysis per week from 30 to 15-20. Similarly, patients on a 5x/weekly dialytic protocol in the Lecce center in Italy showed a significant improvement in anemia after switching from a conventional HD regimen6, with significantly higher hemoglobin and hematocrit.
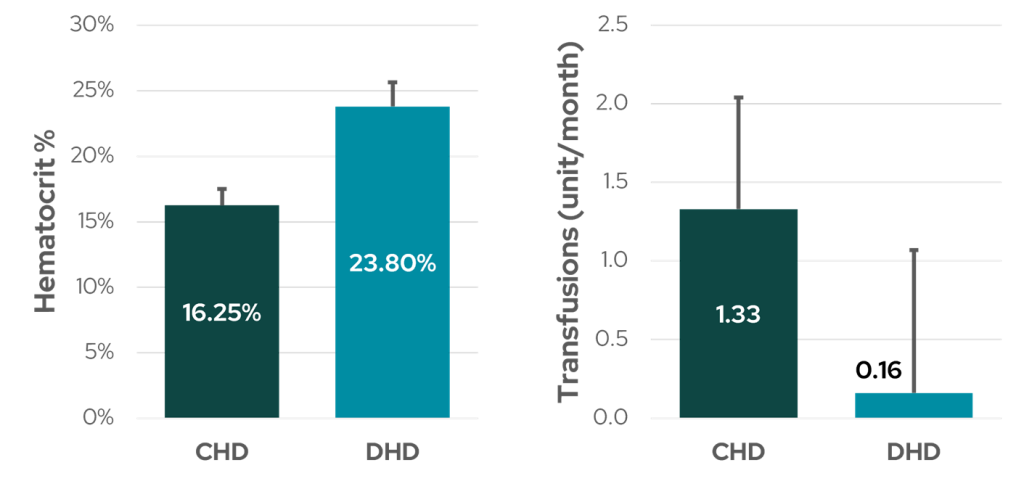
Figure 1: Anemia management in six patients before and after daily dialysis (5x/week). CHD: conventional hemodialysis, DHD: daily hemodialysis (data from Bonomini et al5).
Studies where EPO responsiveness and anemia management have been reported in patients treated with increased dialysis frequency indicate a reduced requirement for EPO (Figure 2) with either maintained hemoglobin or even increased levels (Figure 3).
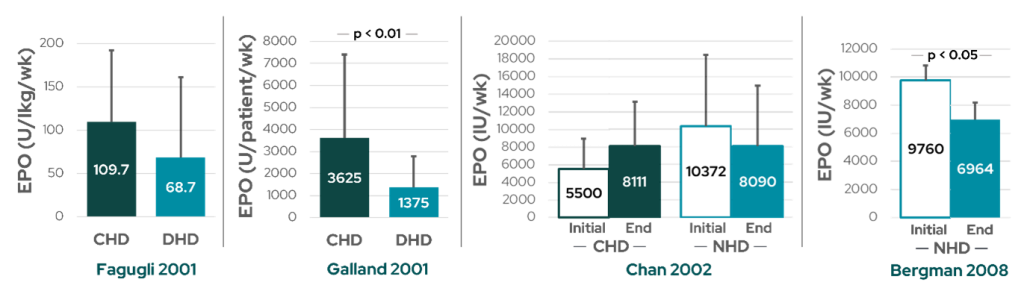
Figure 2: The impact of frequent HD on anemia management with EPO from various studies. There were no differences in EPO treatment between conventional and daily HD in Fagugli et al7 (far left). Galland et al8 reported a 63% reduction in EPO dose for daily HD patients (middle left) while maintaining an adequate hemoglobin level (see Figure 3). Despite a trend toward lower EPO requirements in nocturnal HD patients in Chan et al9 (middle right), hemoglobin increased in this cohort (see Figure 3). Bergman et al1 reported decreased EPO requirements (far right) with a corresponding increase in hemoglobin. CHD: conventional hemodialysis; DHD: daily hemodialysis; NHD: nocturnal hemodialysis.
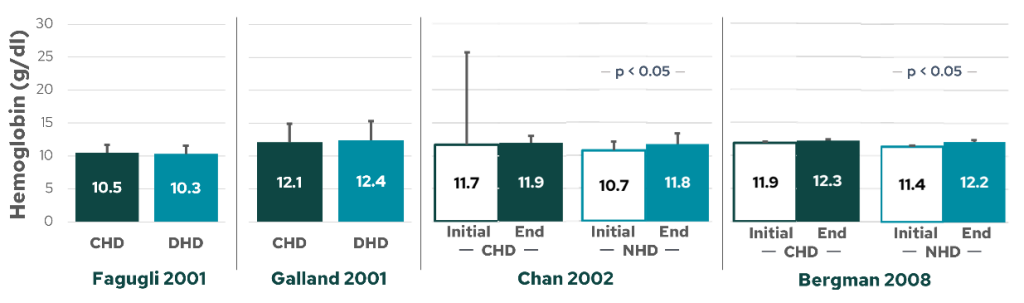
Figure 3: The impact of frequent HD on hemoglobin from various studies. No differences in hemoglobin were reported in Fagugli et al7 (far left) or Galland et al8 (middle left) between conventional and daily HD. However, two following studies showed an increase in hemoglobin concentration after conversion from conventional to nocturnal HD, both Chan et al9 (middle right) and Bergman et al1 (far right). CHD: conventional hemodialysis; DHD: daily hemodialysis; NHD: nocturnal hemodialysis.
In another restrospective controlled study, Poon et al2 investigated whether anemia and ESA requirements are improved in patients receiving alternate nocturnal home HD (NHHD, n = 23) compared to conventional HD patients (n = 25), and importantly, whether these benefits extend beyond the first year of more frequent dialysis.
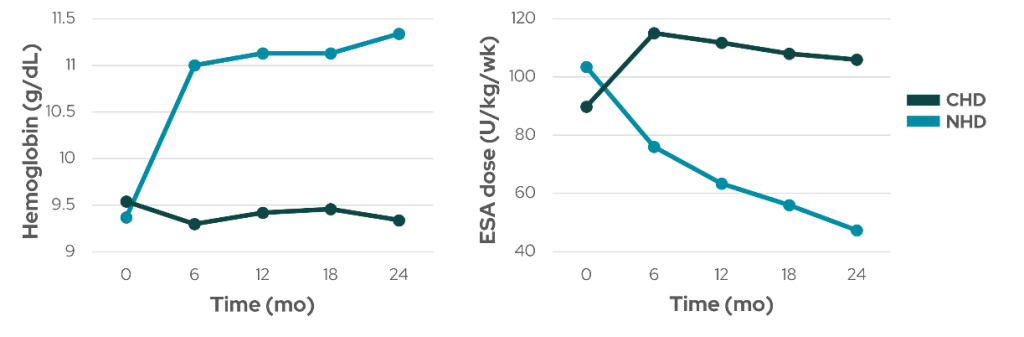
Figure 4: Hemoglobin levels (left) and weekly dose of ESA per kilogram body weight (right) in nocturnal home HD (NHD) and conventional HD (CHD) cohorts over a two-year investigative period (data from Poon et al2).
Hemoglobin level increased significantly by 21% while weekly dose of ESA decreased significantly by 54.2% in the NHD group at the end of two years, with no significant changes in the CHD group (Figure 4). Six out of 23 NHD patients (26%) were able to completely stop ESA treatment. Together, these studies show that more frequent HD may improve anemia control and reduce the need for EPO treatment, likely through increasing the adequacy of dialysis treatment and improving uremic clearance2, but future adequately powered studies are necessary to conclude these beneficial long-term clinical outcomes.
References:
- Bergman A, Fenton SSA, Richardson RMA, Chan CT. Reduction in cardiovascular related hospitalization with nocturnal home hemodialysis. Clin Nephrol. 2008;69(1):33-39. Available from: http://www.ncbi.nlm.nih.gov/pubmed/18218314.
- Poon CKY, Tang H-L, Wong JHS, et al. Effect of alternate night nocturnal home hemodialysis on anemia control in patients with end-stage renal disease. Hemodial Int. 2015;19(2):235-241. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25251291.
- Rioux J-P, Chan CT. Nocturnal home hemodialysis and its impact on erythropoietin responsiveness. Clin Nephrol. 2010;74(3):167-172. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20860900.
- Suri RS, Nesrallah GE, Mainra R, et al. Daily hemodialysis: a systematic review. Clin J Am Soc Nephrol. 2006;1(1):33-42. Available from: http://www.ncbi.nlm.nih.gov/pubmed/17699188.
- Bonomini V, Mioli V, Albertazzi A, Scolari P. Daily-dialysis programme: indications and results. Proc Eur Dial Transplant Assoc. 1972;9(11):44-52. Available from: http://www.ncbi.nlm.nih.gov/pubmed/9829478.
- Mastrangelo F, Alfonso L, Napoli M, DeBlasi V, Russo F, Patruno P. Dialysis with increased frequency of sessions (Lecce dialysis). Nephrol Dial Transplant. 1998;13 Suppl 6:139-147. Available from: http://www.ncbi.nlm.nih.gov/pubmed/9719221.
- Fagugli RM, Reboldi G, Quintaliani G, et al. Short daily hemodialysis: blood pressure control and left ventricular mass reduction in hypertensive hemodialysis patients. Am J Kidney Dis. 2001;38(2):371-376. Available from: http://www.ncbi.nlm.nih.gov/pubmed/11479164.
- Galland R, Traeger J, Arkouche W, Cleaud C, Delawari E, Fouque D. Short daily hemodialysis rapidly improves nutritional status in hemodialysis patients. Kidney Int. 2001;60(4):1555-1560. Available from: http://www.ncbi.nlm.nih.gov/pubmed/11576372.
- Chan CT, Floras JS, Miller JA, Richardson RMA, Pierratos A. Regression of left ventricular hypertrophy after conversion to nocturnal hemodialysis. Kidney Int. 2002;61(6):2235-2239. Available from: https://www.sciencedirect.com/science/article/pii/S0085253815484741.
GMO-001404 Rev B 11/2024