
Effect of Session Duration
The majority of kidney replacement therapy patients around the world receive conventional dialysis for four-hour sessions three times a week. In 2022, 52.6% of US home HD patients were prescribed 3 to 5.9 hours per session per week (Figure 1).
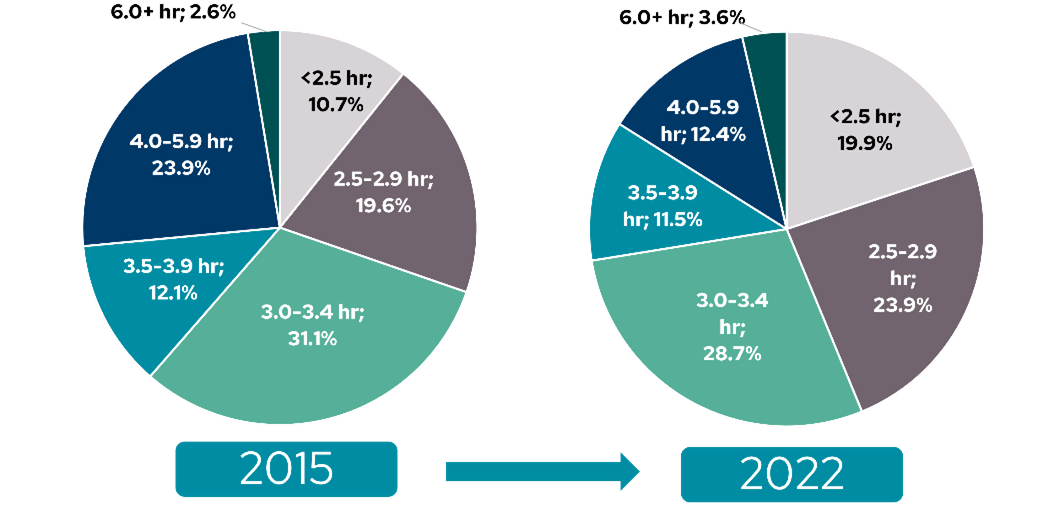
Figure 1: Prescribed number of treatment hours per session in adult patients performing home HD in the US. In 2022, 43.8% were prescribed sessions of less than 3 hours, 40.2% were prescribed sessions of 3.0 to 3.9 hours, 12.4% were prescribed sessions of 4.0 to 5.9 hours, and only 3.6% were prescribed sessions of 6 hours or more, presumably in the context of nocturnal HD (Adapted from USRDS 2024 ADR1 Chapter 2: Home Dialysis. Figure 2.11b).
Although limited clinical trial data exists to inform guidelines for optimal session length, increasing evidence suggests that greater cumulative treatment hours per week, irrespective of home or in-center treatment location, has been associated with improvement in many clinical outcomes. However, it is challenging to disentangle the unique roles of treatment duration and treatment frequency. Nevertheless, current KDOQI guidelines recommend a minimum treatment time of three hours , while acknowledging that many patients require longer session length to achieve adequate dialysis treatment2.
By only including patients on thrice-weekly HD schedules, several observational studies have linked shorter sessions with higher mortality, particularly when HD duration is under four hours3–5.
An early observational study by Charra et al6 in 1992 accredited a remarkably low annual mortality rate of 5% over four years to a longer average treatment length of eight hours in thrice weekly dialysis sessions, claiming that longer session duration resulted in more adequate control of blood pressure through sufficient ultrafiltration. Conversely, in 2000, Gotch et al7 reviewed the survival rate of several large datasets of dialysis patients and found that the two studies with the lowest mortality rates resulted from the longest (8 hours) and shortest (2.3 hours) per-session treatment times, with the remaining studies falling in between. Nonetheless, the annual mortality rate was markedly greater at 14% with 2.3 hour average dialysis session duration, suggesting that session length is still related to survival albeit non-linearly.
Using data from the international Dialysis Outcomes and Practice Patterns Study (DOPPS), two observational studies published evidence supporting better survival of patients receiving longer treatment times in the setting of conventional thrice-weekly HD8,9. Saran et al8 found that longer HD session length and a slower rate of fluid removal (low ultrafiltration rate, UFR) are independently associated with lower mortality and may improve tolerability of treatment. In addition to lower mortality, Tentori et al9 demonstrated an association between longer treatment time and better intermediate outcomes, including lower systolic blood pressure and improvement in blood pressure control, lower risk of hospital admission for fluid overload or congestive heart failure, and better control of anemia and phosphorus levels.
To inform NKF-KDOQI guideline updates, Slinin et al10 performed a systematic review of publications from 2000-2014 including four studies in this time range that specifically evaluated longer session duration11–14, from 4.5 to 8 hours. While there were several improvements detected within individual studies in the longer session duration groups – such as decreased mortality rate and fewer all-cause hospitalizations13, lower systolic BP12, lower left ventricular mass13, and improvement in surrogate markers β2-microglobulin, serum albumin, and serum phosphate – overall, the pooled results found that extended length HD did not improve mortality compared to conventional HD10. Notably, these trials had relatively short follow-up periods, with only one study reporting outcomes surpassing a year11. The Time to Reduce Mortality in ESRD (TiME) trial – a more recent pragmatic randomized clinical trial – was also unable to determine a correlation between thrice-weekly HD session durations of at least 4.25 hours and improved mortality and hospitalization due to insufficient intervention uptake15, although it should be noted that this study used a relatively small increase in treatment time compared to conventional HD. Substantially longer treatment duration, such as the extended-hours HD made possible with nocturnal therapy, has been shown to have a lower risk of mortality than conventional regimens, even with thrice-weekly schedules16.
Combined, these studies offer some support for lengthening treatment duration and suggest that several pathophysiological mechanisms may contribute to the better outcomes observed with longer treatment times independent of any increase in dialysis frequency. Increasing the duration of HD sessions can improve clearance of middle molecules and larger solutes, require less use of phosphate binders, facilitate slower ultrafiltration rates, improve fluid volume and blood pressure control, and reduce cardiovascular morbidity and mortality8,16. These benefits must be considered in the context of patient tolerability of treatment such as the willingness to consistently apply longer therapy, which can have a substantial effect on patient lifestyle. Often, longer treatment times are accomplished through eight-hour nocturnal HD sessions, which may mitigate significant daytime lifestyle changes.
References:
- United States Renal Data System. 2024 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2024.
- National Kidney Foundation. KDOQI Clinical Practice Guideline for Hemodialysis Adequacy: 2015 Update. American Journal of Kidney Diseases. 2015;66(5):884-930.
- Brunelli SM, Chertow GM, Ankers ED, Lowrie EG, Thadhani R. Shorter dialysis times are associated with higher mortality among incident hemodialysis patients. Kidney Int. 2010;77(7):630-636. Available from: http://linkinghub.elsevier.com/retrieve/pii/S0085253815543159.
- Flythe JE, Curhan GC, Brunelli SM. Shorter length dialysis sessions are associated with increased mortality, independent of body weight. Kidney Int. 2013;83(1):104-113.
- Marshall MR, Byrne BG, Kerr PG, McDonald SP. Associations of hemodialysis dose and session length with mortality risk in Australian and New Zealand patients. Kidney Int. 2006;69(7):1229-1236. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16609687.
- Charra B, Calemard E, Ruffet M, et al. Survival as an index of adequacy of dialysis. Kidney Int. 1992;41(5):1286-1291. Available from: http://www.ncbi.nlm.nih.gov/pubmed/1614043.
- Gotch FA, Sargent JA, Keen ML. Whither goest Kt/V? Kidney Int. 2000;58:S3-S18.
- Saran R, Bragg-Gresham JL, Levin NW, et al. Longer treatment time and slower ultrafiltration in hemodialysis: associations with reduced mortality in the DOPPS. Kidney Int. 2006;69(7):1222-1228. Available from: http://linkinghub.elsevier.com/retrieve/pii/S0085253815516335.
- Tentori F, Zhang J, Li Y, et al. Longer dialysis session length is associated with better intermediate outcomes and survival among patients on in-center three times per week hemodialysis: results from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Nephrology, dialysis, transplantation. 2012;27(11):4180-4188. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3529546&tool=pmcentrez&rendertype=abstract.
- Slinin Y, Greer N, Ishani A, et al. Timing of Dialysis Initiation, Duration and Frequency of Hemodialysis Sessions, and Membrane Flux: A Systematic Review for a KDOQI Clinical Practice Guideline. American Journal of Kidney Diseases. 2015;66(5):823-836.
- Lindsay RM, Leitch R, Heidenheim APP, Kortas C, London Daily/Nocturnal Hemodialysis Study. The London Daily/Nocturnal Hemodialysis Study–study design, morbidity, and mortality results. American journal of kidney diseases. 2003;42(1 Suppl):5-12. Available from: http://www.ncbi.nlm.nih.gov/pubmed/12830437.
- McGregor DO, Buttimore AL, Lynn KL, Nicholls MG, Jardine DL. A Comparative Study of Blood Pressure Control with Short In-Center versus Long Home Hemodialysis. Blood Purif. 2001;19(3):293-300. Available from: http://www.ncbi.nlm.nih.gov/pubmed/11244189.
- Ok E, Duman S, Asci G, et al. Comparison of 4- and 8-h dialysis sessions in thrice-weekly in-centre haemodialysis. Nephrol Dial Transplant. 2011;26:1287-1296.
- Wang W, Tonelli M, Hemmelgarn B, et al. The effect of increasing dialysis dose in overweight hemodialysis patients on quality of life: a 6-week randomized crossover trial. Am J Kidney Dis. 2008;51(5):796-803. Available from: http://www.ncbi.nlm.nih.gov/pubmed/18436090.
- Dember LM, Lacson E, Brunelli SM, et al. The time trial: A fully embedded, cluster-randomized, pragmatic trial of hemodialysis session duration. Journal of the American Society of Nephrology. 2019;30(5):890-903. Accessed November 19, 2020
- Rivara MB, Adams S V., Kuttykrishnan S, et al. Extended-hours hemodialysis is associated with lower mortality risk in patients with end-stage renal disease. Kidney Int. 2016;90(6):1312-1320. Accessed March 15, 2023
GMO-001408 Rev B 11/2024