
Reduction of Hospitalizations
Multiple studies have reported fewer hospitalizations for patients treated by frequent home HD compared to conventional thrice weekly treatments, and specifically a lower risk of cardiac-related hospitalization.
Bergman et al1 analyzed and compared 42 patients on conventional HD with 32 patients on frequent nocturnal HD. The patients were well matched for age, gender, ESKD vintage, and controlled for comorbidities, as assessed by the Charlson index. The primary outcomes included admission rate, duration of hospitalization, emergency visits, and dialysis-related biochemical parameters. The authors found that while hospital admission rate was stable for the conventional HD cohort (from 0.48 admission per patient year at baseline to 0.40 at the end of the study), a conversion to frequent nocturnal HD was associated with a decrease in dialysis and cardiovascular-related hospital admission (from 0.50 to 0.17 admissions per patient year, p < 0.05) (Figure 1). There was no significant difference in ER visits between the two cohorts, and a non-significant trend towards shortening of hospitalization duration was seen in both the conventional HD group and the frequent nocturnal HD group.
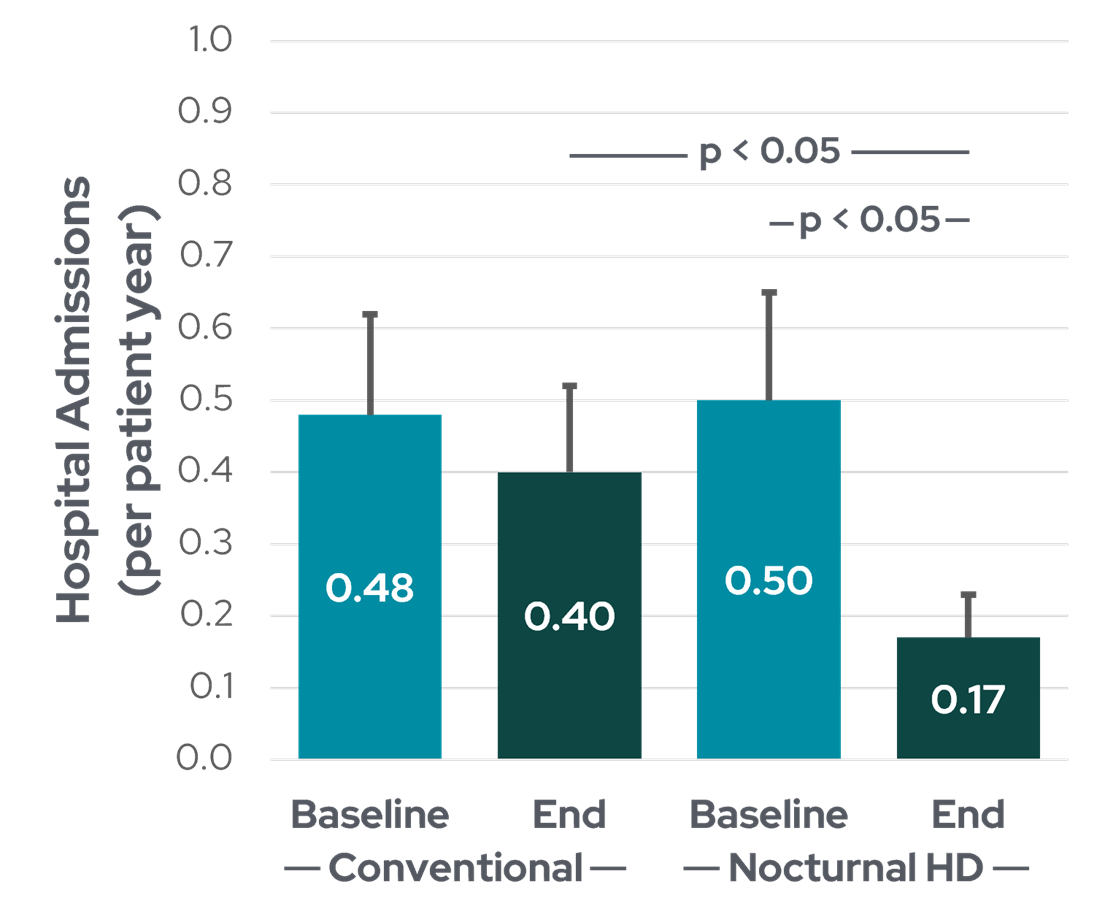
Figure 1: Rate of hospitalization for patients before and after conversion to frequent nocturnal HD (data from Bergman et al1).
In this same study, cardiovascular disease was the principal cause for hospitalization in patients treating with conventional HD, and accounted for 37% of all admissions in this cohort, while 56% of admissions in the frequent nocturnal HD cohort were related to vascular access (p = 0.001). Vascular access-related admission rate remained similar for patients in both cohorts despite a greater proportion of access-related admissions in the frequent nocturnal HD group.
In another study of hospitalization patterns, Zimbudzi et al2 compared the admission rates of 25 HHD patients (8 hour sessions, every other day) with 25 satellite HD patients (5 hour sessions, thrice weekly). The authors found that HHD patients spent 14 days less in the hospital compared to satellite HD patients (2.8 vs 3.4 days/patient-year, p < 0.005). They also reported a non-significant reduction in length of stay (0.8 of a day difference) in favor of the HHD group and an equal number of admissions (0.72 admissions/patient-year) for both cohorts.
In an observational cohort study published the following year, Weinhandl et al3 used registry data to investigate whether daily HHD is associated with a lower hospitalization risk5. The authors examined records from 3,480 patients prescribed 5-6 home HD sessions per week and 17,400 thrice-weekly ICHD patients and found that while all-cause hospitalization risk was similar in both cohorts (Hazard Ratio, HR: 1.01; 95% CI, 0.98-1.03), the risk of cardiovascular-related admission was significantly lower with frequent HHD (HR: 0.89; 95% CI, 0.86-0.93), for first admission and readmission. The authors also reported that the risk of first admission was higher with daily HHD (HR: 1.14; 95% CI, 1.09-1.19) while the risk of readmission was slightly lower (HR:0.96; 95% CI, 0.94-0.99), and that the risk of infection-related admission with daily HHD was higher (HR: 1.18; 95% CI, 1.13-1.23)3.
These findings were confirmed by another observational retrospective cohort study by Suri et al4 in the same year that matched registry data from 1187 daily HHD patients with 3173 ICHD controls. Similarly, the authors found that while there was no significant difference in hospitalizations between daily HHD and ICHD patients (0.93 vs. 1.10/patient-year, HR: 0.92; 95% CI, 0.85-1.00, p = 0.053), cardiovascular hospitalizations were lower with daily HHD than with ICHD (HR: 0.68; 95% CI, 0.61-0.77, p < 0.001).
Overall, the protective association of frequent HHD with cardiovascular-related hospitalizations in these studies is particularly noteworthy, given that cardiovascular disease remains the leading cause of death in hemodialysis patients. Frequent hospital admissions pose the risk of further debilitation or mortality for patients and impacts their quality of life2,4, in addition to posing a financial burden for health institutions2. In-patient care for hospitalized HD patients has been identified as one of the costliest elements of treatment5, and as such, the reduction in hospital resource utilization with home therapy could have major implications for the cost of health care for dialysis patients and programs.
References:
- Bergman A, Fenton SSA, Richardson RMA, Chan CT. Reduction in cardiovascular related hospitalization with nocturnal home hemodialysis. Clin Nephrol. 2008;69(1):33-39. Available from: http://www.ncbi.nlm.nih.gov/pubmed/18218314.
- Zimbudzi E, Samlero R. How do hospitalization patterns of home hemodialysis patients compare with a reasonably well dialysis patient cohort? Int J Nephrol Renovasc Dis. 2014;7:203-207. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=4051731&tool=pmcentrez&rendertype=abstract.
- Weinhandl ED, Nieman KM, Gilbertson DT, Collins AJ. Hospitalization in daily home hemodialysis and matched thrice-weekly in-center hemodialysis patients. American Journal of Kidney Diseases. 2015;65(1):98-108.
- Suri RS, Li L, Nesrallah GE. The risk of hospitalization and modality failure with home dialysis. Kidney Int. 2015;88(2):360-368.
- Lee H, Manns B, Taub K, et al. Cost analysis of ongoing care of patients with end-stage renal disease: the impact of dialysis modality and dialysis access. Am J Kidney Dis. 2002;40(3):611-622. Available from: http://www.ncbi.nlm.nih.gov/pubmed/12200814.
GMO-001406 Rev B 11/2024