
Cardiovascular Outcomes
Cardiovascular disease is the leading cause of death in patients with chronic kidney disease treated with dialysis, and increased left ventricular (LV) mass, also known as LV hypertrophy, is an important predictor of cardiovascular morbidity and mortality in this population1–4. High blood pressure, or hypertension, and interdialytic weight gain, are associated with LV hypertrophy, are also prevalent in patients with chronic kidney disease, and are known risk factors that further contribute to cardiovascular disease5,6. Intensive HD regimens may normalize blood pressure (BP) and regress LV hypertrophy compared to conventional thrice weekly HD (Figure 1), allowing many patients to reduce or even discontinue their antihypertensive medications3,7–12. While not all of the studies presented here were performed in the home setting, the implications of the improved outcomes associated with more frequent hemodialysis apply to home hemodialysis as this setting is the most convenient treatment location to increase dialysis frequency and adhere to an intensified prescription.
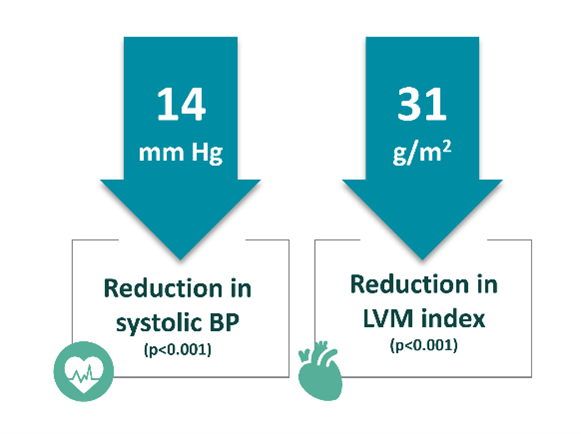
Figure 1: In a meta-analysis of frequent or extended hemodialysis, Susantitaphong et al3 demonstrated that these HD regimens reduced both systolic blood pressure (35 study arms, 928 patients) and LV mass index (23 study arms, 524 patients).
In his study of 12 patients transferred from three to six times weekly HD, Fagugli et al7 measured blood pressure by 24-hour ambulatory measurements and cardiac dimensions by echocardiography and found that daily HD allowed optimal control of BP and reduced left ventricular mass (LVM) index. The authors reported a significant reduction in 24-hour systolic BP from 148 to 128 mm Hg, diastolic BP from 73 to 67 mm Hg, and an LVM index decrease from 148.7 to 120.1 g/m2 (Figure 2). Notably, the decrease in SBP and LVM index was correlated with the reduction in extracellular water (SBP: r = 0.63; p<0.01; LVMi: r=0.66; p<0.01), and permitted seven of the eight patients to discontinue the use of antihypertensive medications.
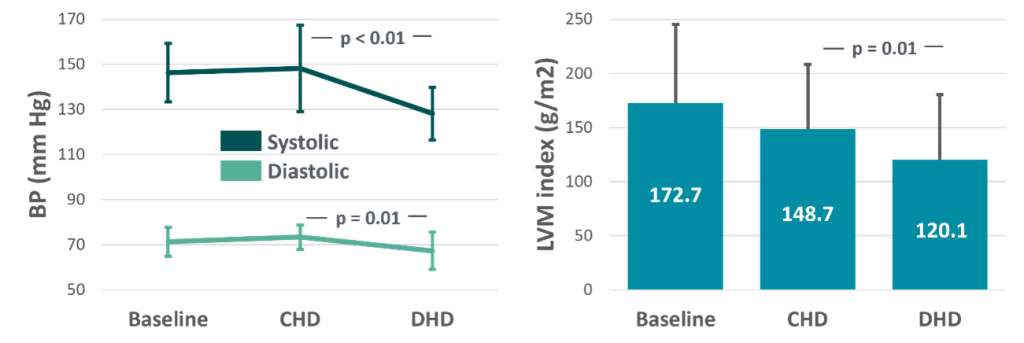
Figure 2: 24-hour systolic BP and diastolic BP (left), and LVM index (right) decreased when patients switched from conventional, thrice weekly (CHD) to short daily HD (DHD) (data from Fagugli et al7).
In a study conducted by Chan et al11, the impact on LVH and BP was assessed when 28 patients were transferred from conventional HD (four hours, thrice weekly) to frequent nocturnal HD (8-10 hours, 6-7 times per week). Compared to 13 patients remaining on conventional HD, the authors reported decreased systolic and diastolic BP despite a reduction in antihypertensive medication and a significant decrease in LV mass index (Figure 3).
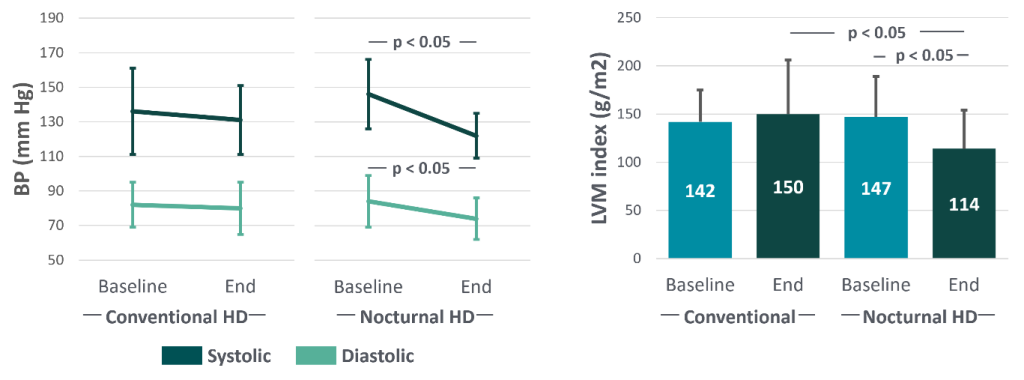
Figure 3: Systolic BP and diastolic BP (left), and LVM index (right) decreased when patients switched from conventional HD to frequent nocturnal HD (data from Chan et al11).
The Frequent Hemodialysis Network (FHN) Trial was a multicenter, randomized controlled trial with both a daily and nocturnal arm designed to evaluate mortality, cardiovascular, and quality of life outcomes. In the daily trial, patients were randomly assigned to undergo conventional HD (3 treatments per week, 2.5-4 hours per session) or frequent HD (6 treatments per week, 1.5-2.75 hours per session)8. In this study, both cohorts performed HD treatments in-center, but the implications of the improved outcomes in the frequent HD patients are relevant given that home is the most convenient treatment location for patients to increase dialysis frequency and adhere to an intensified prescription.
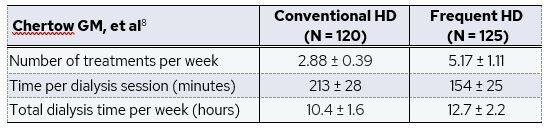
Nearly 95% of patients in the conventional HD group had adherence over 80% while only 77.7% on frequent HD had adherence over 80%. Nevertheless, patients randomly assigned to frequent HD had favorable cardiovascular outcomes, including an LV mass decrease of 16.4 ± 2.9 g (relative to a 2.6 ± 3.1 g decrease in the conventional hemodialysis group; difference, -13.8 g, p < 0.001), and a weekly average pre-dialysis systolic BP decrease of 9.2 ± 1.5 mm Hg in the frequent HD group after adjustment for baseline (compared to a 0.9 ± 1.6 mm Hg increase in the conventional HD group; difference -10.1 g, p < 0.001)8.
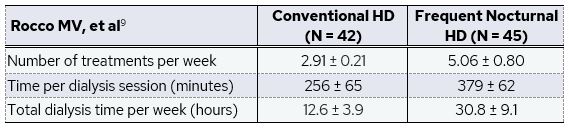
In the nocturnal trial, patients were randomly assigned to undergo conventional HD (3 treatments per week) or frequent nocturnal HD (6 treatments per week)9. In this arm of the study, both the conventional and frequent HD treatments were performed primarily at home. Near 98% of patients in the conventional HD group attended at least 80% of dialysis treatments in a given month, while only 72.7% on frequent nocturnal HD had adherence over 80%.
In this study, frequent nocturnal HD significantly improved systolic BP, but did not result in substantial improvements in LV mass. After adjusting for baseline, weekly average pre-dialysis systolic BP decreased by 9.8 ± 2.7 mm Hg in the nocturnal HD group and decreased by 0.1 ± 2.6 mm Hg in the conventional HD group (difference: -9.7 g, p = 0.009). LV mass decreased by 9.2 ± 4.6 g in the nocturnal group, compared to a 1.7 ± 4.5 g increase in the conventional hemodialysis group (difference: -10.9 g, p = 0.09)9. The trend towards an improvement in LV mass is in line with the statistically significant improvement reported in the Daily FHN trial but did not reach significance in the Nocturnal FHN trial, possibly due to the relatively small patient sample size and lower adherence to the dialysis prescription, both of which reduced the power of the study.
In another randomized controlled trial, Culleton et al12 recruited 52 patients and randomly assigned individuals to receive nocturnal HD six times per week (minimum 6 hours/night, 30-48 hours weekly) or conventional HD three times per week (10.5-13.5 hours weekly). The authors measured change in LV mass by cardiovascular magnetic resonance imaging, with secondary outcomes including blood pressure and medication use. They found that frequent nocturnal HD significantly reduced mean LV mass by 13.8 ± 23 g in the nocturnal group, compared to a 1.5 ± 24 g increase in the conventional hemodialysis group (difference: 15.3g, p = 0.04). Antihypertensive medication use was reduced or discontinued in 16 of 26 patients randomized to nocturnal HD and only 3 of 25 patients randomized to conventional HD (p<0.001). Despite this reduction, six-month systolic BP decreased in nocturnal HD patients by 7 mm Hg and increased in conventional HD patients by 4 mm Hg (after adjusting for baseline, difference: 14 mm Hg, p= 0.01)12.
To directly compare the effect of both frequent treatment schedules within a single center, the London Daily/Nocturnal Hemodialysis study assessed mean arterial blood pressure (MAP) and intensity of antihypertensive therapy in 11 patients on short daily HHD and 12 patients on long nocturnal HHD, where each patients had a matched control treated by conventional ICHD5. Consistent with other studies, both regimens of increased frequency HHD were associated with significant lowering of MAP and reduced antihypertensive tablets consumed, while matched controls had no change in MAP and an increase in antihypertensives use5.
Combined, these studies show that the two approaches to increasing dialysis frequency – short daily and long nocturnal – both effectively improve BP management and reverse LV hypertrophy. Through improving blood pressure and LV hypertrophy, more frequent HD – facilitated through home therapy – may reduce cardiovascular morbidity and mortality.
References:
- United States Renal Data System. 2023 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2023.
- Collins AJ, Foley RN, Gilbertson DT, Chen S-C. The State of Chronic Kidney Disease, ESRD, and Morbidity and Mortality in the First Year of Dialysis. Clinical Journal of the American Society of Nephrology. 2009;4(Supplement_1):S5-S11.
- Susantitaphong P, Koulouridis I, Balk EM, Madias NE, Jaber BL. Effect of Frequent or Extended Hemodialysis on Cardiovascular Parameters: A Meta-analysis. American Journal of Kidney Diseases. 2012;59(5):689-699.
- Sarnak MJ, Auguste BL, Brown E, et al. Cardiovascular Effects of Home Dialysis Therapies: A Scientific Statement From the American Heart Association. Circulation. 2022;146(11):E146-E164. Available from: https://pubmed.ncbi.nlm.nih.gov/35968722/.
- Nesrallah G, Suri R, Moist L, Kortas C, Lindsay RM. Volume control and blood pressure management in patients undergoing quotidian hemodialysis. Am J Kidney Dis. 2003;42(1 Suppl):13-17. Available from: http://www.ncbi.nlm.nih.gov/pubmed/12830438.
- Reaves AC, Weiner DE, Sarnak MJ. Home Dialysis in Patients with Cardiovascular Diseases. Clinical Journal of the American Society of Nephrology. Published online February 6, 2024.
- Fagugli RM, Reboldi G, Quintaliani G, et al. Short daily hemodialysis: blood pressure control and left ventricular mass reduction in hypertensive hemodialysis patients. Am J Kidney Dis. 2001;38(2):371-376. Available from: http://www.ncbi.nlm.nih.gov/pubmed/11479164.
- Chertow GMG, Levin NNW, Beck GGJ, et al. In-center hemodialysis six times per week versus three times per week. N Engl J Med. 2010;363(24):2287-2300. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21091062.
- Rocco M V., Lockridge RS, Beck GJ, et al. The effects of frequent nocturnal home hemodialysis: the Frequent Hemodialysis Network Nocturnal Trial. Kidney Int. 2011;80(10):1080-1091. Available from: https://www.ncbi.nlm.nih.gov/pubmed/21775973.
- Bergman A, Fenton SSA, Richardson RMA, Chan CT. Reduction in cardiovascular related hospitalization with nocturnal home hemodialysis. Clin Nephrol. 2008;69(1):33-39. Available from: http://www.ncbi.nlm.nih.gov/pubmed/18218314.
- Chan CT, Floras JS, Miller JA, Richardson RMA, Pierratos A. Regression of left ventricular hypertrophy after conversion to nocturnal hemodialysis. Kidney Int. 2002;61(6):2235-2239. Available from: https://www.sciencedirect.com/science/article/pii/S0085253815484741.
- Culleton BF, Walsh M, Klarenbach SW, et al. Effect of Frequent Nocturnal Hemodialysis vs Conventional Hemodialysis on Left Ventricular Mass and Quality of Life. JAMA. 2007;298(11):1291. Available from: http://jama.jamanetwork.com/article.aspx?doi=10.1001/jama.298.11.1291.
GMO-001399 Rev A 11/2024