
Effect of Frequency
There is an increasing wealth of research suggesting that numerous clinical and lifestyle benefits are associated with more frequent hemodialysis (>4 sessions per week) when compared to conventional, three times per week dialysis, assuming the patient is receiving at least a minimal dose of therapy.
Assessing adequacy of more frequent treatments is better quantified using the weekly standard Kt/V (stdKt/V), which is a linear function, rather than equilibrated Kt/V (eKt/V), which is a logarithmic function (Figure 1).
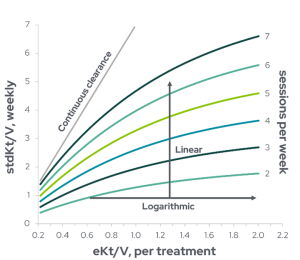
Figure 1: Graphical model depicting the relationship between equilibrated Kt/V (eKt/V) delivered for each dialysis session (values on the x-axis) and weekly standard Kt/V achieved (values on the y-axis). The number of sessions per week are shown on the right side and correspond to different line colors. eKt/V is described as a logarithmic function, while stdKt/V is a linear function. The continuous clearance line shown is the eKt/V values multiplied by seven and represents the weekly stdKt/V with continuous dialysis (Adapted from Gotch et al1).
A fundamental observation comparing frequency and outcomes was the similar survival of patients undergoing continuous peritoneal dialysis with a relatively low Kt/V on a daily basis to patients on thrice weekly HD with much higher Kt/V1,2. As visualized by Figure 2, the eKt/V for thrice weekly HD is 1.1 and for continuous ambulatory peritoneal dialysis (CAPD) is 0.3, both corresponding to an adequate weekly stdKt/V of 2.0. As such, there is close agreement between the recommended dialysis dose for CAPD and for thrice weekly HD when expressed as stdKt/V.
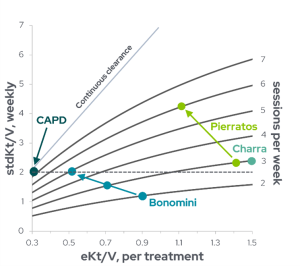
Figure 2: Distribution of stdKt/Vs calculated for three studies of dialysis with frequency four to six times per week, depicting relationship between eKt/V delivered for each dialysis and weekly standard Kt/V, with the number of sessions per week shown on the right side. Multiple dots are shown for studies that reported results from increasing weekly frequency (Adapted from Gotch et al1, with individual studies: Bonomini 19983, Pierratos 19984, Charra 19925.)
Figure 2 also illustrates the eKt/V and stdKt/V calculated for several studies in which patients were treated with more frequent dialysis, with frequencies ranging from four to six times per week1. Bonomini et al3 compared patients undergoing HD from two to five times per week, with a low eKt/V but an effectively higher stdKt/V due to the increased frequency, finding that persistent symptoms of uremia – including severe anemia, uncontrolled hypertension, pericarditis, peripheral neuropathy, insomnia, and restless leg syndrome – were reduced or eliminated with more HD sessions per week. Although there was minimal change in weekly summed eKt/V in these patients, there was a marked increase in stdKt/V from 1.2 with two sessions per week to 2.2 with five sessions per week. Similarly, Pierratos et al4 reported high patient satisfaction, improved energy and stamina, and clinical improvements such as stabilized BP and reduced antihypertensive medication when hemodialysis frequency was increased from thrice weekly (Kt/V = 1.26) to six to seven times per week (Kt/V = 0.99). Finally, Mastrangelo et al6 observed a 60% survival at 10 years and 48% at 16 years with every other day hemodialysis (4 times/week) with an average weekly Kt/V of 4.62 (per treatment Kt/V ranged from 1.06-1.25). Many recent studies have corroborated this early evidence, showing that frequent hemodialysis is associated with improved survival, reduced hospitalizations, significant cardiovascular improvement, improved recovery time, and many quality of life benefits7–9. Findings from these studies are further detailed in the “Benefits of Home Hemodialysis” section.
Challenges with thrice-weekly hemodialysis
The intermittent nature of HD leads to large fluctuations in volume status and electrolyte balance, starting with the prolonged chronic hemodynamic period of extracellular fluid accumulation and overload followed by the accelerated intravascular fluid depletion induced during the HD session10. With the majority of patients still prescribed a conventional thrice weekly HD regimen, the average hemodialysis patient goes through an unnatural cyclical interdialytic fluid loading (between treatments, ~44-68 hours) and intradialytic unloading (during treatments, ~4 hours) process. The longest interdialytic interval occurs most commonly through a weekend, when patients have two days instead of the usual one day without dialysis, resulting in large interdialytic weight gains (up to 7 kg11). Unsurprisingly, this yields an uneven distribution of sudden and cardiac deaths throughout the week, with a 23% higher death rate following the “two-day gap12.”
Bleyer et al11 reported a marked increase in all-cardiac deaths among patients on thrice weekly HD on the Monday following a weekend without dialysis, and for patients on a Tuesday-Thursday-Saturday schedule, there was a significant increased proportion of all cardiac deaths on Tuesday (Figure 3).
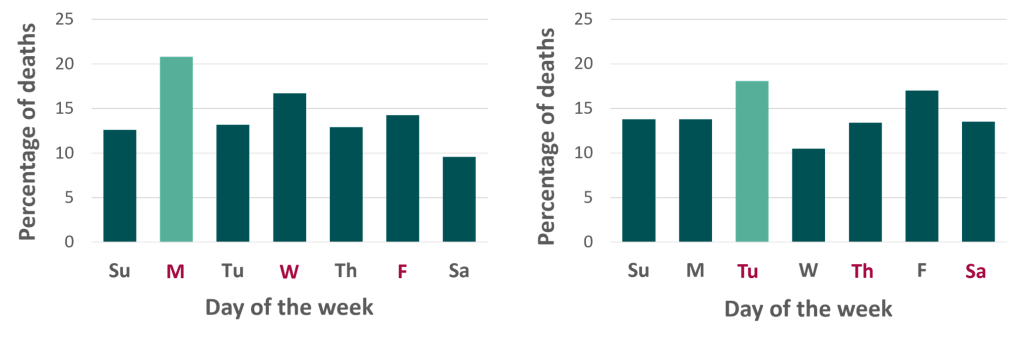
Figure 3: Distribution of all cardiac deaths according to the day of the week for a Monday, Wednesday, and Friday dialysis schedule (left), and a Tuesday, Thursday, Saturday dialysis schedule (right), (Adapted from Bleyer et al11).
In addition to the increased mortality due to fluid and toxin accumulation during the two-day interval, removal of large amounts of fluid during the first dialysis session following the longest interval results in post-dialysis hypotension, which can have severe consequences in a patient population that already commonly has underlying cardiovascular disease11. In a following study, Bleyer et al13 expanded on the unphysiological profile of HD delivery by reporting a 1.7-fold increased risk of death in the 12-hour period starting with the dialysis procedure and a three-fold increased risk of death in the 12 hours before dialysis at the end of the weekend interval (Figure 4).
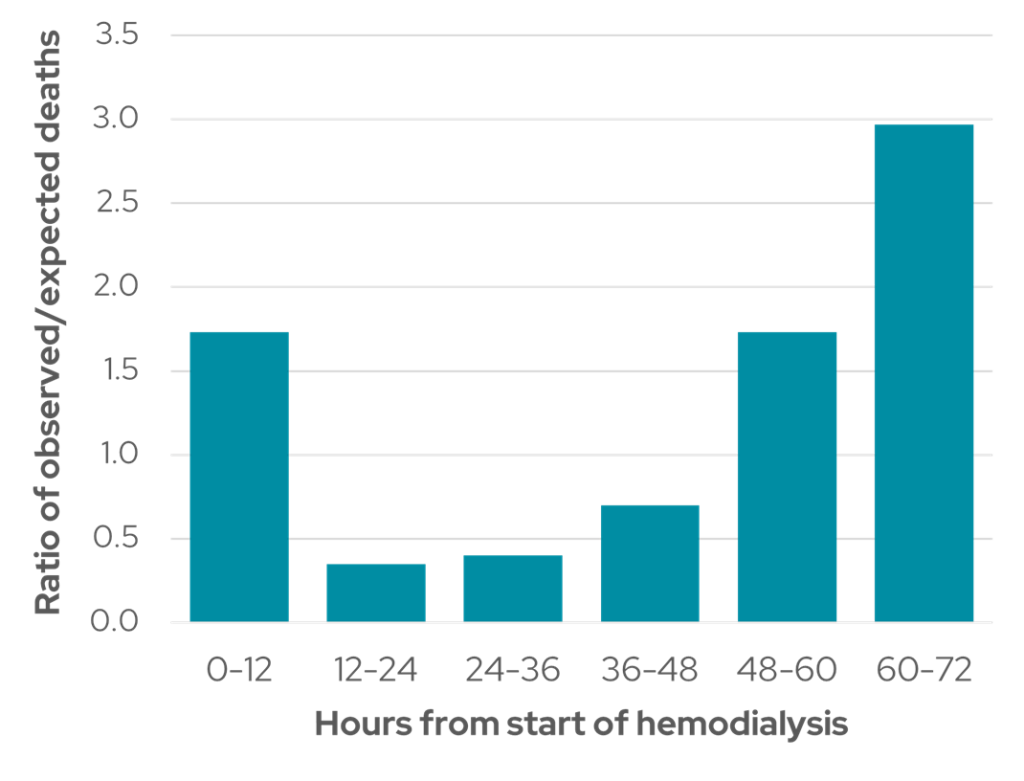
Figure 4: Distribution of sudden death in relation to hours from start of hemodialysis (Adapted from Bleyer et al13).
Mortality is therefore temporally related to both hemodynamic stress phases of the HD procedure, the short intradialytic period and the extended interdialytic phase. More frequent HD treatment could be beneficial in alleviating some of this burden11.
Following a two-day gap, patients also experience the highest cardiovascular-related hospitalization rates (124% higher12). Intermittent HD may increase morbidity due to either excessive fluctuations in volume resulting in a progressive increase in arterial hypertension, cardiac strain and ventricular hypertrophy, and pulmonary congestion, or by the accumulation of solutes in critical concentrations, such as hyperkalemia from elevated potassium (Figure 5).
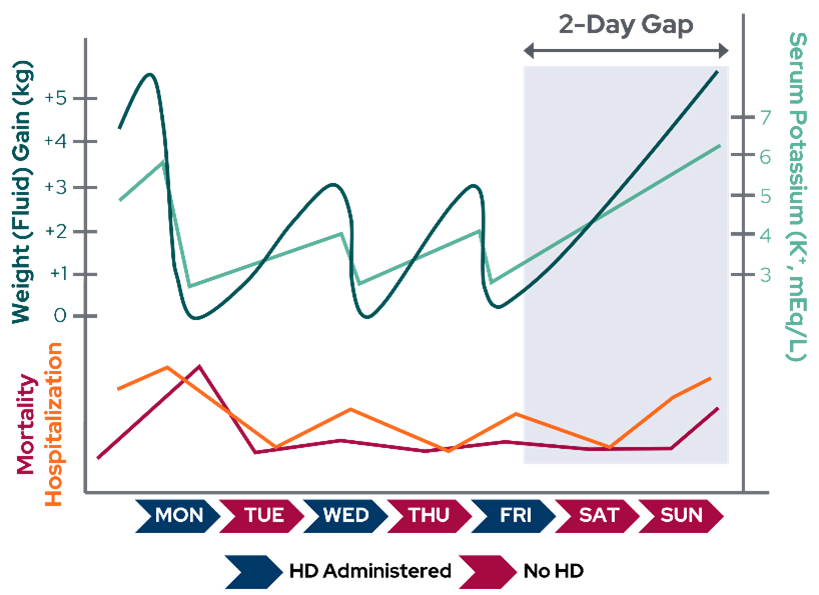
Figure 5: Theoretical fluid (blue) and electrolyte (green) fluctuations in a patient receiving HD treatment three times per week on Monday, Wednesday, and Friday. Lower line graphs depict higher mortality (red) and hospitalizations (orange) after the two-day gap (Adapted from Rhee et al14).
Published studies of patients receiving hemodialysis more than three times per week make a strong case for frequent therapy and suggest that these regimens provide improved urea kinetics and dynamics and biochemical, hemodynamic, clinical, and nutritional benefits compared to the conventional HD prescription.
In the next sections, we will cover specific evidence-based improvements in clinical outcomes with frequent hemodialysis, schedules which are easier to adhere to when the patient performs treatment in the home setting.
References:
- Gotch FA, Sargent JA, Keen ML. Whither goest Kt/V? Kidney Int. 2000;58:S3-S18.
- Diaz-Buxo JA. Beyond thrice-weekly hemodialysis. Hemodial Int. 2005;9(3):309-313. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16191082.
- Bonomini V, Mioli V, Albertazzi A, Scolari P. Seminal contribution to dialysis. Daily-dialysis programme: indications and results. Nephrology Dialysis Transplantation. 1998;13(11):2774-2777.
- Pierratos A, Ouwendyk M, Francoeur R, et al. Nocturnal hemodialysis: three-year experience. J Am Soc Nephrol. 1998;9(5):859-868. Available from: http://www.ncbi.nlm.nih.gov/pubmed/9596084.
- Charra B, Calemard E, Ruffet M, et al. Survival as an index of adequacy of dialysis. Kidney Int. 1992;41(5):1286-1291. Available from: http://www.ncbi.nlm.nih.gov/pubmed/1614043.
- Mastrangelo F, Alfonso L, Napoli M, DeBlasi V, Russo F, Patruno P. Dialysis with increased frequency of sessions (Lecce dialysis). Nephrol Dial Transplant. 1998;13 Suppl 6:139-147. Available from: http://www.ncbi.nlm.nih.gov/pubmed/9719221.
- Chertow GMG, Levin NNW, Beck GGJ, et al. In-center hemodialysis six times per week versus three times per week. N Engl J Med. 2010;363(24):2287-2300. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21091062.
- Jaber BL, Lee Y, Collins AJ, et al. Effect of daily hemodialysis on depressive symptoms and postdialysis recovery time: Interim report from the FREEDOM (Following Rehabilitation, Economics and Everyday-Dialysis Outcome Measurements) Study. American Journal of Kidney Diseases. 2010;56(3):531-539. Available from: https://pubmed.ncbi.nlm.nih.gov/20673601/.
- Tennankore KK, Chan CT, Curran SP. Intensive home haemodialysis: benefits and barriers. Nat Rev Nephrol. 2012;8(9):515-522.
- Canaud B, Stephens MP, Nikam M, Etter M, Collins A. Multitargeted interventions to reduce dialysis-induced systemic stress. Clin Kidney J. 2021;14(Suppl 4):i72-i84. Available from: https://pubmed.ncbi.nlm.nih.gov/34987787/.
- Bleyer AJ, Russell GB, Satko SG. Sudden and cardiac death rates in hemodialysis patients. Kidney Int. 1999;55(4):1553-1559. Available from: http://www.ncbi.nlm.nih.gov/pubmed/10201022.
- Foley RN, Gilbertson DT, Murray T, Collins AJ. Long Interdialytic Interval and Mortality among Patients Receiving Hemodialysis. New England Journal of Medicine. 2011;365(12):1099-1107. Available from: http://www.nejm.org/doi/abs/10.1056/NEJMoa1103313.
- Bleyer AJ, Hartman J, Brannon PC, Reeves-Daniel A, Satko SG, Russell G. Characteristics of sudden death in hemodialysis patients. Kidney Int. 2006;69(12):2268-2273. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16672908.
- Rhee CM, Chou JA, Kalantar-Zadeh K. Dialysis Prescription and Sudden Death. Semin Nephrol. 2018;38(6):570-581.
GMO-001406 Rev B 4/2025