
Acute Kidney Care
Introduction
Acute kidney injury (AKI) is generally recognized as an abrupt decline in kidney function. Definitions have varied over the past few decades. AKI definitions consist of three diagnostic parameters: an increase in serum creatinine, a decrease in urine output, and the need for kidney replacement therapy (KRT). Specifically, an increase in serum creatinine (SCr) by ≥0.3 mg/dL within 48 hours, an increase in SCr ≥1.5 times baseline within the past seven days, or a urine volume <0.5 ml/kg/h for 6 hours indicate AKI. Severity of AKI is categorized by stages 1-3 according to the Kidney Disease Improving Global Outcomes (KDIGO) guidelines, which is a combination of RIFLE (Risk, Injury, Failure, Loss of kidney function, and End-stage kidney disease) and AKIN (Acute Kidney Injury Network) criteria (see table 1). A patient should be staged according to the worst stage criteria that they meet. Determining the stage that a patient meets involves an evaluation. Physical examination is an important step that allows the evaluator to determine fluid status, as well as signs and symptoms such as edema or dry mucous membranes. A computed tomography (CT) scan, renal ultrasonography, and/or a renal biopsy may help determine the cause of AKI. Metabolic acidosis and electrolyte abnormalities (i.e., potassium, phosphorus, calcium) may be present upon laboratory workup as well (1).
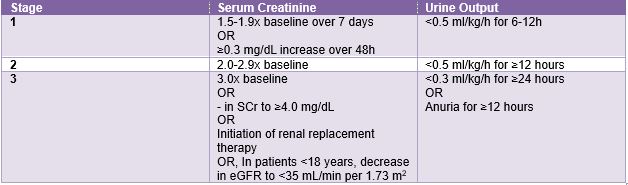
Table 1. Stages of AKI, adapted from KDIGO Guidelines (2)
Epidemiology
In the United States, AKI has increased fourfold over the past several decades. AKI is responsible for complicating 5-7% of acute-care hospital admissions and up to 30% of cases admitted to the intensive care unit (ICU). Additionally, AKI contributes to an increase in morbidity and mortality in hospitalized patients (3). Some risk factors for AKI include diabetes, chronic kidney disease, albuminuria, heart or liver disease, advanced age, and certain medications (1).
Pathophysiology
Common causes of AKI include sepsis, ischemia, acute pancreatitis, and chemotherapeutic agents (3). There are three categories of causes of AKI: prerenal, intrinsic, and postrenal (see image 1). Prerenal AKI is due to decreased renal perfusion. Decreased renal perfusion refers to reduced blood flow to the kidneys. There are different etiologies for decreased renal perfusion which may include hypovolemia, hypotension, renal vasoconstriction, or glomerular efferent arteriolar vasodilation. Intrinsic renal causes are due to an injury to the glomerulus or tubule. Examples of these injuries are acute tubular necrosis, acute interstitial nephritis, and glomerulonephritis. Lastly, postrenal causes are due to an obstruction. This could be a blood clot, tumor, or urethral obstruction (4).
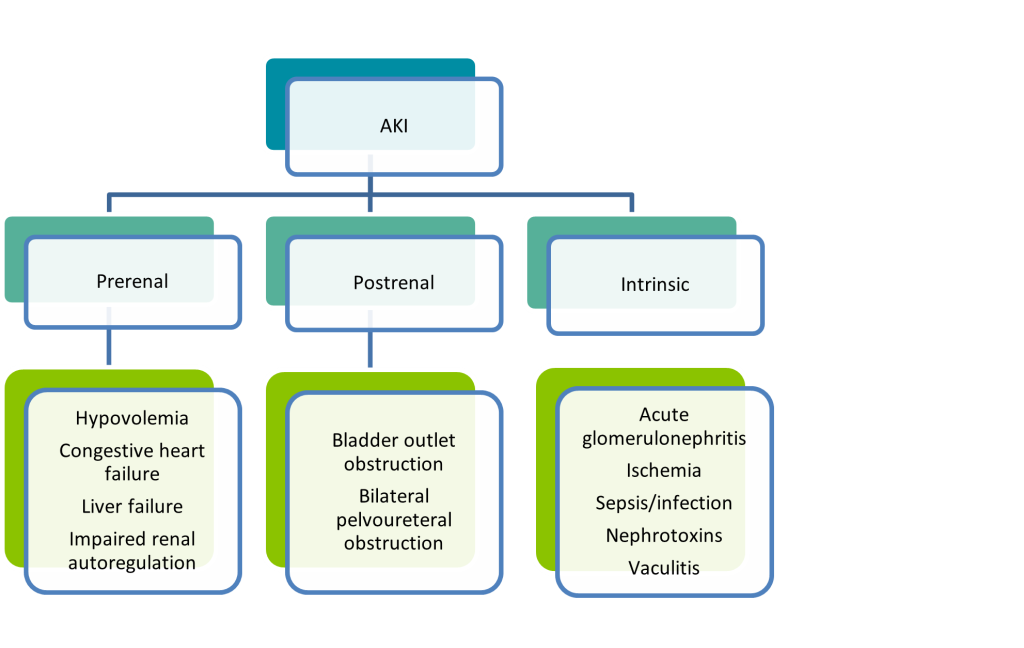 Image 1. Causes of AKI (3)
Image 1. Causes of AKI (3)
Symptomatology
Patients with AKI may vary in clinical presentation. Signs and symptoms may include changes in urinary output, flank pain, edema, and weight changes. Patient assessment is an important part of evaluating the patient, which involves looking at the patient’s medical history, chronic conditions, and medications. Although patients with chronic kidney disease already have decreased kidney function, a drastic increase in their baseline SCr can still be used as an indicator of an acute injury (1). Severe AKI includes signs of pulmonary edema or patients not responding to hyperkalemia treatment (4).
Outcomes
As mentioned previously, a rise of ≥0.3 mg/dL in SCr has been associated with a higher mortality, and AKI has been associated with an increased risk of death. The main treatment goal for AKI is to minimize kidney injury as much as possible (1, 3). An important part of this is maintaining the individual’s fluid level requirements and considering comorbidities. Additionally, avoiding hypotension by targeting a mean arterial pressure of 65-85 mmHg helps with prevention and treatment of AKI. Lastly, ensuring adequate nutritional support is important to help improve survival (5).
Complications
The most common complications of AKI include hyperkalemia, metabolic acidosis, and hyperphosphatemia. Edema (pulmonary and peripheral) can arise as well due to fluid overload. Fluid overload can lead to heart failure. Gastrointestinal effects such as nausea/vomiting are common. Additonally, neurologic effects are a complication which includes cognitive impairment and lethargy (4).
Treatment and Management
The first step to treating AKI is determining if the cause is pre-renal or intrinsic by performing a fluid challenge (4). A fluid challenge involves administering fluids and monitoring the response using urine output. For patients with pre-renal AKI, the fluid challenge will result in improved renal function. For patients that do not respond to the fluid challenge, reassessment or a nephrology consult is recommended. If patients are experiencing fluid overload and have heart failure, then loop diuretics such as intravenous furosemide are recommended for treatment. If the patient has fluid overload without heart failure, a nephrology consult is recommended (5). Optimizing medication regimens is important in managing the condition of these patients. It is important to avoid nephrotoxic medications, as well as renally adjusting the medications the patient is currently taking. For a patient with hyperkalemia, there are many treatment options that can be used. Those options include dietary restriction, insulin, intravenous (IV) dextrose, potassium-binding resins, calcium gluconate, and lastly, dialysis. Additionally, some patients may require adjustments for metabolic abnormalities. For instance, a patient experiencing metabolic acidosis would require monitoring of blood pH and bicarbonate administration (4). Kidney replacement therapies may also be necessary when treatings these patients. Kidney replacement therapies can be intermittent or continuous. For patients who are hemodynamically unstable, continuous kidney replacement is preferred (1). While a patient is undergoing kidney replacement therapy, monitoring is essential. Patients should be evaluated daily in the inpatient setting, and weekly while in the outpatient setting regarding continuing kidney replacement therapy (4).
In summary, AKI is an important condition that should be recognized and treated as soon as possible in patients. There are multiple etiologies of AKI, so patients with risk factors should be carefully monitored and managed. Current management strategies include correcting fluid overload, avoiding nephrotoxic medications, and treating electrolyte and metabolic abnormalities. When unrecognized and untreated, AKI can lead to many complications including the development or worsening of chronic kidney disease and even death.
References:
- Maker J, Roller L, Dager W. Chapter 61: Acute Kidney Injury. In: DiPiro’s Pharmacotherapy: A Pathophysiologic Approach. 12th ed. McGraw-Hill Education; 2023. https://accesspharmacy.mhmedical.com/content.aspx?sectionid=269666129&bookid=3097&Resultclick=2#1197548749. Accessed April 19, 2023.
- Kidney International. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney International Supplements. 2012;2(1). https://kdigo.org/wp-content/uploads/2016/10/KDIGO-2012-AKI-Guideline-English.pdf. Accessed April 21, 2023.
- Waikar S, Bonventre J. Chapter 310: Acute Kidney Injury. In: Harrison’s Principles of Internal Medicine. 21st ed. McGraw Hill; 2022.
- Goyal A, Daneshpajouhnejad P, Hashmi M, Bashir K. Acute Kidney Injury. National Library of Medicine. https://www.ncbi.nlm.nih.gov/books/NBK441896/. Published January 2023. Accessed April 25, 2023.
- Kher V, Srisawat N, Noiri E, et al. Prevention and Therapy of Acute Kidney Injury in the developing world. Kidney International Reports. 2017;2(4):544-558. doi:10.1016/j.ekir.2017.03.015
GMO-000829 Rev A 04/2024