
Nutrition
Malnutrition is a frequent problem in maintenance HD patients and is an important factor influencing morbidity and mortality. Several studies have suggested that more frequent HD, either in the form of short daily HHD or long nocturnal HHD, improves appetite and nutritional parameters due to liberalized fluid and dietary restrictions and improved general well-being1–6.
The effect of converting 17 patients from standard HD (4-5 hour sessions, thrice weekly) to short daily HD (2-2.5 hour sessions, six times weekly) on nutritional parameters including dietary measures, anthropometry, and biochemical evaluations (serum albumin, prealbumin). Dietary protein and calorie intake was calculated from dietary history, and normalized protein equivalent of nitrogen appearance (nPNA) was calculated from urea kinetic modeling. The authors reported that more frequent dialysis dramatically increased appetite and food intake of patients4,6, with significant increases in daily protein intake and an accompanying increase in dry body weight and lean body mass (Figure 1). Biochemical indicators of nutrition – mean serum albumin, prealbumin, and total cholesterol – also increased significantly after starting more frequent HD4,6. Galland et al4 speculated that frequent HD might improve appetite due to improved general well-being, reduced post-dialysis fatigue, fewer dietetic rules, liberalized sodium and water intake, reduced urea retention, and reduced fluid overload.
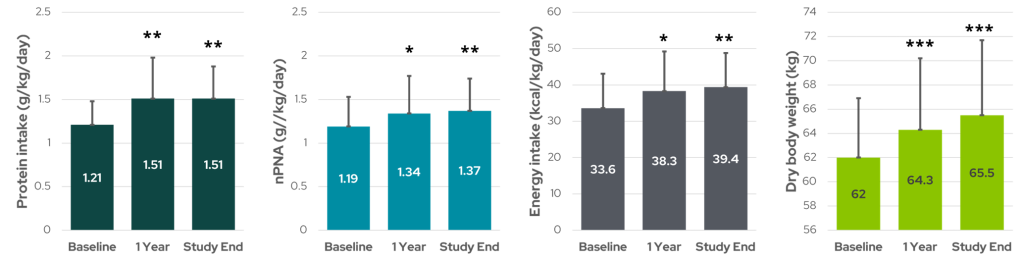
Figure 1: Nutritional parameters including dietary protein intake and normalized protein equivalent nitrogen appearance (nPNA) (two on left), energy intake (middle right), and dry body weight (far right) during 12 months of short daily HD. * denotes p < 0.05, ** p < 0.01, and *** p < 0.001 (data from Galland et al6).
Changes in nutritional status were also examined in the London Daily/Nocturnal Hemodialysis study, which compared patients receiving frequent home HD – either short daily (n=11) or long nocturnal (n=12) – with 22 matched control patients receiving conventional thrice weekly HD3. Like Galland et al., this study measured several biochemical parameters indicative of nutritional status, including nPNA, serum albumin and prealbumin, and body composition data. Control patients showed no significant change in nPNA, serum albumin, or mid-arm muscle area (a measure of lean body mass). However, for daily HD patients, the authors reported increased nPNA, serum albumin levels, and arm muscle area, suggestive of improved nutritional status. There was no comparable improvement observed in nocturnal HD patients, and even a decline in serum albumin. However, the frequent nocturnal data are far from conclusive and may be confounded by the 50% patient drop out in this group3. While interpretation should be guarded, it does appear that the improved nutritional status for short daily HD is consistent with that reported by Galland et al.
In another study of nocturnal HHD, Sikkes et al2 examined the effect of 8 hour nocturnal HD sessions six times weekly on various nutritional parameters. In this single-center, prospective, nonrandomized study, 14 patients who were stable on conventional HD were converted to nocturnal home HD and followed for one year while measuring appetite, protein, mineral, and fluid intake, changes in body weight, and biochemical data. Patients could follow a free diet and drink more, and maintained detailed dietary records to track their nutrient intake. The authors found that appetite increased in around half of the patients during the first year on nocturnal HHD, and body weight and body mass index significantly increased as a result. Protein intake in grams per day and relative to body weight increased as well and was evident as early as 3 months after beginning more intensive treatment (Figure 2). Normalized Protein Catabolic Rate (nPCR) increased without reaching statistical significance (p = 0.058), although in 8 of 14 patients, where the baseline nPCR was less than 1 g/kg/day, nPCR doubled after one year (p = 0.012). Serum phosphate, calcium, and potassium intake increased by 25% or more within 3 months of treatment, but concentrations of these minerals remained the same in laboratory results2.
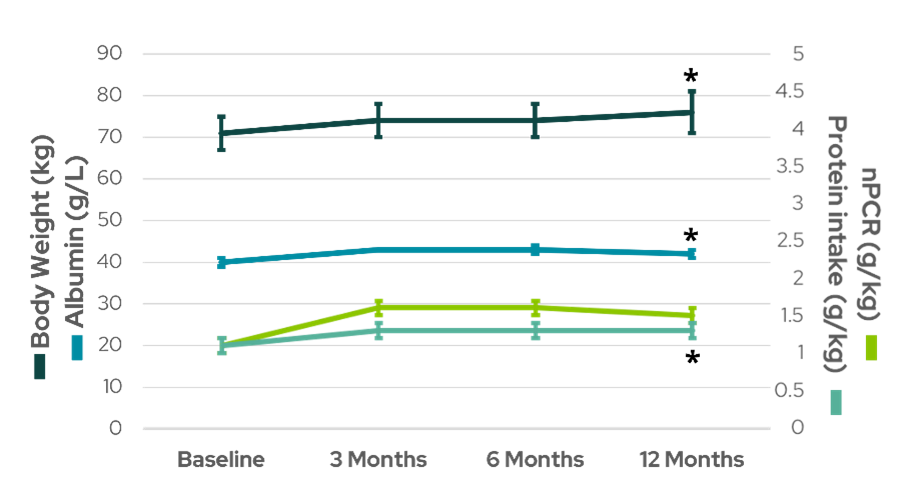
Figure 2: Body weight, serum albumin, and protein intake increased significantly after one year of nocturnal HHD (data from Sikkes et al2).
Although not all studies report improved nutritional status in patients undergoing frequent HD5, there exists a plethora of evidence suggesting more frequent dialysis with a liberalized diet and fewer fluctuations in fluid levels and solute concentrations results in increased appetite, protein and calorie intake, and gains in dry body weight and muscle mass, with favorable changes often occurring just weeks after increasing dialysis frequency2,3,6,7.
References:
- Pierratos A, Ouwendyk M, Francoeur R, et al. Nocturnal hemodialysis: three-year experience. J Am Soc Nephrol. 1998;9(5):859-868. Available from: http://www.ncbi.nlm.nih.gov/pubmed/9596084.
- Sikkes ME, Kooistra MP, Weijs PJM. Improved nutrition after conversion to nocturnal home hemodialysis. J Ren Nutr. 2009;19(6):494-499. Available from: http://www.ncbi.nlm.nih.gov/pubmed/19616453.
- Spanner E, Suri R, Heidenheim APP, Lindsay RM. The impact of quotidian hemodialysis on nutrition. American Journal of Kidney Diseases. 2003;42(1 Suppl):30-35. Available from: http://www.ncbi.nlm.nih.gov/pubmed/12830441.
- Galland R, Traeger J, Arkouche W, Cleaud C, Delawari E, Fouque D. Short daily hemodialysis rapidly improves nutritional status in hemodialysis patients. Kidney Int. 2001;60(4):1555-1560. Available from: http://www.ncbi.nlm.nih.gov/pubmed/11576372.
- Suri RS, Nesrallah GE, Mainra R, et al. Daily hemodialysis: a systematic review. Clin J Am Soc Nephrol. 2006;1(1):33-42. Available from: http://www.ncbi.nlm.nih.gov/pubmed/17699188.
- Galland R, Traeger J. Short Daily Hemodialysis and Nutritional Status in Patients with Chronic Renal Failure. Semin Dial. 2004;17(2):104-108.
- Williams AW, Chebrolu SB, Ing TS, et al. Early clinical, quality-of-life, and biochemical changes of “daily hemodialysis” (6 dialyses per week). Am J Kidney Dis. 2004;43(1):90-102. Available from: http://www.ncbi.nlm.nih.gov/pubmed/14712432
GMO-001405 Rev B 11/2024